It’s back, people. It slipped in when we had our guard down. We had a good run there of feeling like life was getting back to normal. We have been out and around, flying without masks, gathering at parties, going to concerts. Most of us are vaccinated now, even boosted once or twice. The fear of the vaccine has decreased as more and more people miraculously survive the shot (it’s safe, really!). We are less nervous to be around strangers as it is now more likely they are vaccinated. Additionally, many of us have had Covid19 this year (2022), so we have embraced our natural immunity. But guess what? It turns out BA.5 doesn’t care. It is taking us down.
The latest Covid19 Omicron strain, BA.5, was discovered in South Africa earlier this year. Spreading faster than the speed of light, it is now the most prevalent strain in the U.S. just a month after gracing our shores. Mayo Clinic just called it “hypercontagious”. Confirming our suspicions, a new study published in Nature this week (see all refs below) found that BA.5 is four times more resistant to our current vaccines than any other previous strain. These variants are different due to mutations in the spike proteins which make it more difficult for the antibodies (that many of us carry against Covid19) to neutralize (stop) the virus.
It’s still worse for the unvaccinated. According to Dr Gregory Polland, head of Mayo Clinic’s Vaccine Research Group:
“… among the unvaccinated with this variant, they’re about fivefold more likely to get infected than people who have been vaccinated and boosted, about 7½ times more likely to be hospitalized, and about 14 to 15 times more likely to die if they get infected.”
Dr Poland also notes that even though vaccinated people are more likely to get mild to moderate symptoms from BA.5, they are still well protected against hospitalization. As before, even with vaccination, there are still high risk populations who have a really hard time with this virus and may quickly develop severe symptoms. Hospitalizations are up 23% just in the past week and have doubled since May. There are still people dying every day in our country due to Covid19, though not at the same rate we saw with previous variants. We always see cases peak, then hospitalizations, then deaths. We don’t know, yet, what the impact of BA.5 will be. (See Florida reference below–they have had BA.5 for a while and are now seeing an increase in deaths). The other challenging part of recent statistics is that so many people are doing home tests. A positive home test doesn’t show up in the local and national numbers. This means that we actually have no idea what the current rate of infection is — it might be much higher than we think.
The best way to prevent getting sick at all is to put a mask on. In my hospital, masks are still required in all hallways and clinical (patient) areas– we never stopped wearing them. Based on CDC guidelines, however, I did stop wearing my mask out in public. Of course, as soon as I went on my first trip without a mask (a dude ranch in Arizona!), I came home with Omicron. I thought I would be safe after vaccination and a booster, but I was very wrong. Since then, I have even had a second booster — about 90 days after my infection. I’m disappointed to hear that BA.5 might still get me despite all of that!
CDC guidance has been confusing and has changed so many times that many people have given up trying to follow the current guidelines.

© 2022 TRIBUNE CONTENT AGENCY. ALL RIGHTS RESERVED.
If you are one of those people, then let me get you up to date with the current recommendations. Instead of putting the whole country on lockdown at once, the CDC has now officially recognized that different areas of the country are seeing surges in infection at different times. Because of this, they now have an easy tool and traffic light warning system for people to follow depending on where they live.
As an example, I live in Washoe County in the state of Nevada. I can go to the CDC website: https://www.cdc.gov/coronavirus/2019-ncov/your-health/covid-by-county.html
I pick “Nevada” on their drop down menu, then “Washoe County”, and I currently find this:
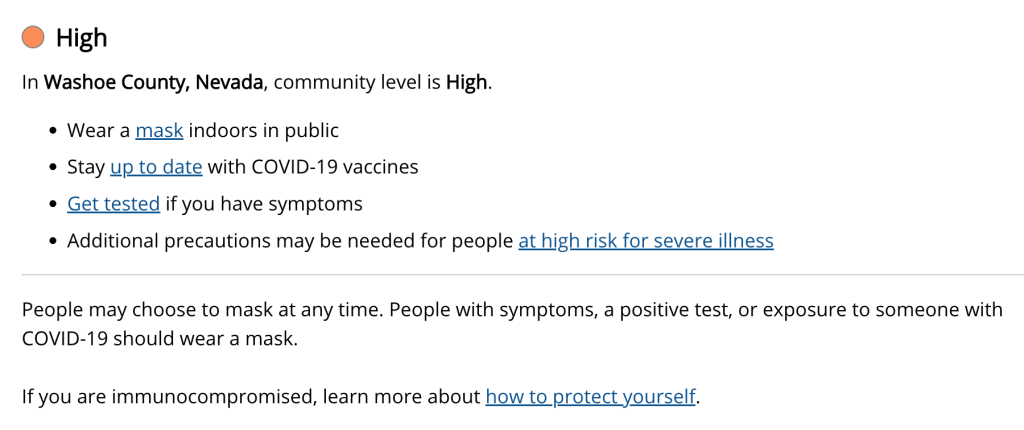
On the same website, you can see the three levels of recommendation which are determined by evaluating the number of Covid cases being reported to the local county health department, the number of local hospital beds being used, and the number of hospital admissions. These are the current traffic lights depending on the level of activity in your county:

It’s a good idea to check this website before you travel. I might be more comfortable walking into a restaurant without a mask in a town that is “green” then in my current neighborhood.
My last thought today – this is HARD. We’ve had our masks off in Washoe County for a long time. Now, I’m putting it back on to go to Walmart or waiting at the airport. I had Covid in February, and it kicked my ass. I really don’t want it again. There are many cases of people who had Covid in March and April getting BA.5 now and getting just as sick as the first time around. I repeat, I don’t want it again. So, I put on my mask and dust off my bottles of hand sanitizer to carry around again. I don’t need anyone else to tell me to do this. I can see the writing on the wall.
I also do this so that I don’t get my elderly parents sick or anyone else around me that might not have the nice immune system that I have. We know that we can spread Covid a day before we even get symptoms. I feel like it is inevitable at this point to get Covid every once in a while, but I don’t want to be responsible for getting someone else really sick. I will wear my mask again.
Please “like” or comment with any questions or concerns. Share with others who need all of this info summarized every once in a while! Let me know what you would like to hear more about, and I will do my best to post about it. Thanks for reading and for all of your support!
References:
Wang, Q., Guo, Y., Iketani, S. et al. Antibody evasion by SARS-CoV-2 Omicron subvariants BA.2.12.1, BA.4, & BA.5. Nature (2022).
https://www.nature.com/articles/s41586-022-05053-w
https://newsnetwork.mayoclinic.org/discussion/what-you-need-to-know-about-the-ba-5-omicron-variant/
https://www.cdc.gov/coronavirus/2019-ncov/your-health/covid-by-county.html